

Introduction
Thoracoabdominal aortic aneurysms (TAAA) represent a unique pathology that is associated with considerable mortality if untreated. While the advent of endovascular technologies has introduced new modalities for consideration, the mainstay of TAAA treatment remains open surgical repair. However, the optimal conduct of open TAAA repair requires careful consideration of patient risk factors and a collaborative team effort to mitigate the risk of perioperative complications. In this article preoperative preparation and operative techniques for open TAAA repair is described.
Preoperative Preparation
- Patients with severe chronic obstructive pulmonary disease, as suggested by a forced expiratory volume in 1 second of less than 0.8 L/min and a partial pressure of carbon dioxide greater than 45 mm Hg, should be evaluated by a pulmonologist and receive bronchodilators as well as pulmonary rehabilitation before repair.
- Preoperative renal function is a strong predictor of postoperative mortality after TAAA repair, and glomerular filtration rate is more sensitive than serum creatinine in predicting postoperative outcomes.
Operative Techniques for Open TAAA Repair
Anesthesia and Monitoring
After induction of general anesthesia, the patient is intubated with a double-lumen endotracheal tube. A large-bore, central, and venous catheter was placed for rapid infusion along with a Swan-Ganz catheter for cardiac evaluation, and nasal and bladder temperatures for core temperature was monitored. Renal temperature is obtained later in the operative field using a needle-probe after exposing the retroperitoneal space. Electroencephalogram, somatosensory evoked potential (SSEP), and motor evoked potential (MEP) are also placed at this point.
Positioning, Incision, and Exposure
The patient should be positioned with the scapulars at a right angle to the edge of the operating table, stabilized by a bean bag, with both axillae well padded. The hips are tilted 60 degrees so that both femoral arteries are accessible (Figure 1).

Figure 1. Positioning and skin incision. Note the scapulars are at 90 degrees to the table but hips are rotated for abdominal and femoral exposures. Adapted from source.
Left Heart Bypass
The left inferior pulmonary vein is used to drain the left heart bypass. On exposure of the left inferior pulmonary vein, the pericardium is opened posteriorly to the left phrenic nerve.
An advantage of using a left heart bypass is the ability to maintain proximal pressure above 100 mm Hg and distal pressure above 60 mm Hg. In addition, the presence of an inline heat exchanger allows the patient to be effectively warmed during the later stages of the procedure.
Proximal Anastomosis
The proximal clamp is placed either proximally or distally to the left subclavian artery, depending on the presence of atheromatous debris and aortic dissection. Sequential clamping of the distal aorta is used to minimize the ischemic insults to the viscera, kidneys, and spinal cord.
Distal Anastomosis, Intercostal Artery Reattachment, and Visceral/Renal Artery Reconstruction
The proximal clamp is now on the graft just distal to the anastomosis, and the distal clamp is moved to the end of the descending aorta. The remaining thoracic aorta is further opened.
There are three methods of intercostal reattachment:
- Loop reconstruction using a 14-mm Dacron graft connected to the main body Dacron graft in a side-to-end and side-to-side fashion to the intercostal artery of half loop for small number of pairs (Figure 2);
- Side-to-side reconstruction by creating a side hole in the main Dacron tube graft and anastomosing to the intercostal arteries as an island; and
- End-to-end reconstruction using an interposing 12-mm by 14-mm Dacron tube graft between the main Dacron graft and each pair of intercostal arteries.
If signal changes are observed early during the clamp period, the important patent intercostal arteries within T8 through T12 are reattached immediately. Loop reconstruction was began using as it seems to reduce the risk of graft thrombosis compared with direct end-to-end anastomosis from a side-arm graft. Otherwise, the reattachment can be performed with distal anastomosis and weaning off pump prior to protamine reversal.
The distal clamp is released to fill the graft with blood and evacuate the graft of all air and debris by placing the patient in the head-down position. The proximal clamp is slowly released to flush the graft in a prograde manner. In cases of Marfan syndrome or other connective tissue disorders in patients younger than 60 years of age, or with ostial separation of greater than 3 cm, a premanufactured side-branched thoracoabdominal aortic graft (STAG) is used with separate bypasses to each of the vessels (Figure 3).
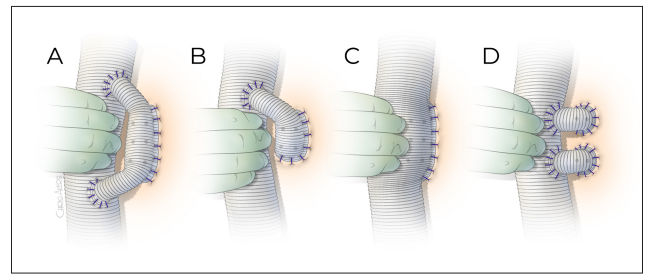
Figure 2. Intercostal artery reattachment techniques. (A) A 14-mm Dacron graft is anastomosed to the anterolateral surface of the main body graft as a loop to reconstruct the intercostal arteries in side-to-end fashion. (B) Similar to the loop graft but the proximal end may not be anastomosed back to the main body graft if reconstructing less than three pairs of intercostal arteries. The anastomosis to the intercostal arteries is performed in end-to-end fashion by beveling the 14-mm graft. (C) A side hole is made large enough to accommodate the intercostal arteries to be reattached and anastomosed as an island patch in side-to-side fashion. (D) A 12-mm ×14-mm Dacron graft is used to reattach each pair of intercostal arteries in an end-to-end fashion. Adapted from source.

Figure 3. Extent II thoracoabdominal aortic aneurysm repair with side-branched thoracoabdominal aortic graft (STAG). Adapted from source.
Hemostasis and Closure
Meticulous attention to hemostasis is mandatory and reduces coagulopathy. It is also important to interrogate the anastomoses. To prevent coagulopathy, hemostasis of muscle edges during thoracoabdominal incision should be managed prior to heparinization. All the mural thrombus in the aorta should be removed to search for intercostal arteries or small branches with patent orifice—and these should be ligated as they may later start to bleed.
Conclusion
The current standard practice of TAAA repair includes: perioperative CSF drainage; left heart bypass with mild hypothermia or cardiopulmonary bypass with moderate/deep hypothermia; sequential clamping; visceral and renal perfusion using roller pump; and aggressive reattachment of patent intercostal arteries within T8 – T12. It is demonstrated that the use of DAP and CSF drainage, in combination with moderate passive hypothermia, has reduced the overall spinal cord ischemia rate after extent I TAAA from 15% to less than 2%, and after extent II TAAA from 33% (50% with clamp time exceeding 40 minutes in “clamp and go” era) to less than 4%.